The associate-to-principal transition: what actually surprised people who have done it
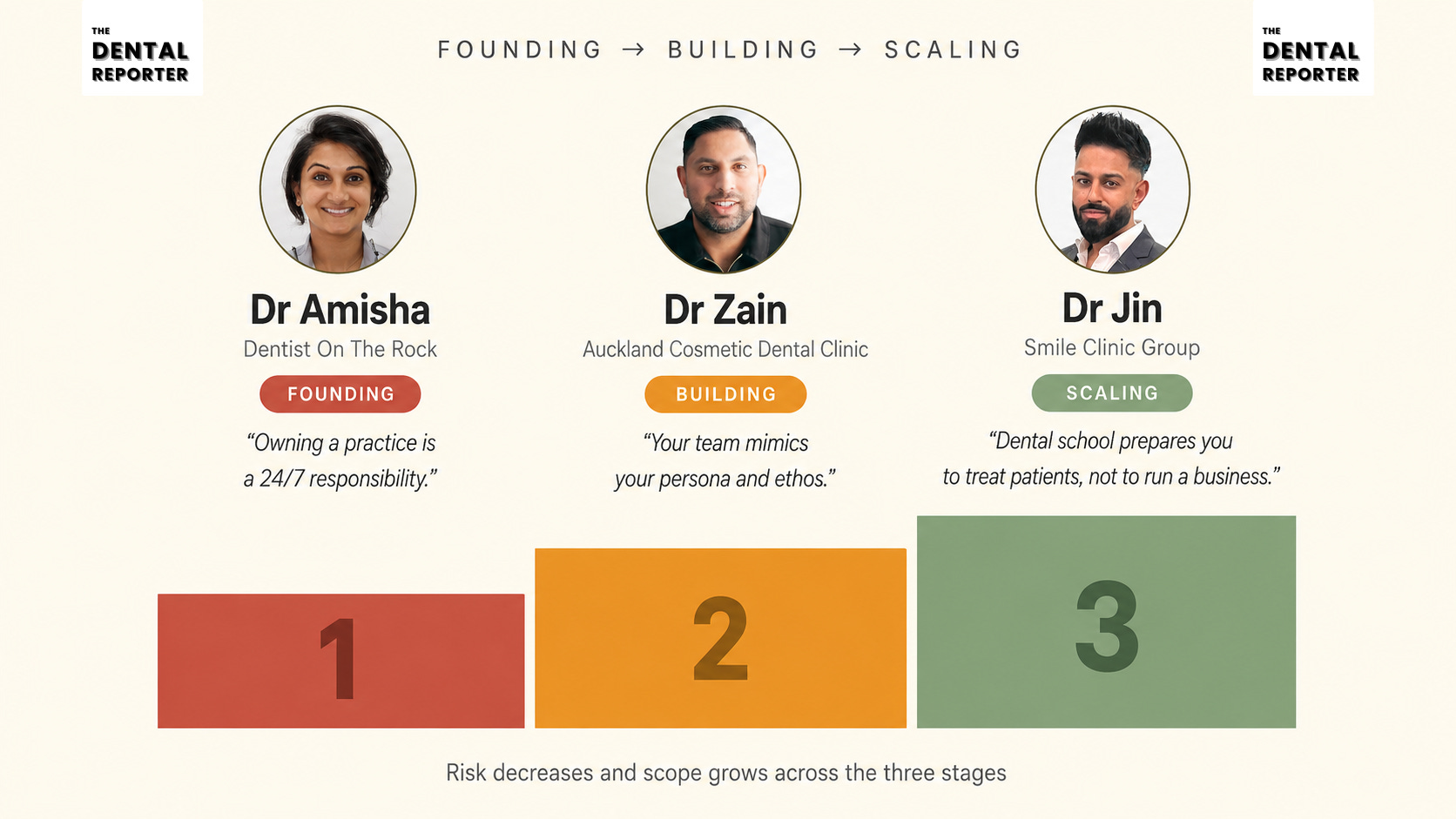
From a first surgery four months in to a 300-person group, the path from associate to owner has stages. Three principals map what each one actually demands.

Ownership is often reduced to a checklist: heads of terms, CQC registration, a change of provider notification, a new set of insurance policies. None of that checklist explains what happens once the ink dries. Three UK principals, each at a different point in that journey, describe what caught them off guard once the legal work was done. Dr Amisha is four months into ownership at Dentist On The Rock, still working through the gap between what she projected and what the practice actually costs to run. Further along sits Dr Zain, at the helm of Auckland Cosmetic Dental Clinic, navigating the shift in patient trust that comes with a change of owner. Dr Jin sits further still: he became a principal at 23 and now leads more than 300 people across Smile Clinic Group, a scale of responsibility few associates ever picture. Their accounts do not agree on everything, but together they map a journey with distinct stages, each carrying its own risk and its own lesson.
Contributors
Dr Jin, CEO & Founder, Smile Clinic Group
Dr Zain, Principal Dentist, Auckland Cosmetic Dental Clinic
Dr Amisha, Principal Dentist, Dentist On The Rock



Founding: the costs nobody put in the plan
At four months in, Dr Amisha is still learning what ownership actually costs. As an associate, she tracked lab bills, materials and treatment costs and assumed she understood outgoings. Ownership introduced a longer list: waste collection, National Insurance, staff pensions, even a charge for banking the practice’s own cash. “The number of invoices that have to be paid, for services you don’t even think of, did catch me off guard,” she says. Budgets have helped less than expected. Fixed costs are straightforward to plan for. The variable ones, an air conditioning repair one month, an equipment failure the next, demand constant attention and a standing contingency.
The team brought a separate lesson. Dr Amisha recognised early that she had inherited a strong team and made keeping them a priority. She held a one-to-one with every member to understand their frustrations and expectations before changing anything. Not every request could be actioned, and some could not be at all, but the exercise shaped which changes were made and when. What she wishes she had understood earlier sits in the numbers: cash flow, staffing costs, KPIs and the systems that keep a practice running. Those are the things she is now learning on the job. There is a quieter warning too. “Owning a practice is a 24/7 responsibility,” she says, and she wishes she had taken more time off before stepping into it.
Building: trust, inspections, and a lesson in due diligence
Dr Zain, Auckland Cosmetic Dental Clinic, is further along the same road, and the surprises at his stage look different. The first was less about money than about people. Patient allegiance, he found, does not transfer automatically from the outgoing owner. That shift felt uncomfortable in the early months and led to encounters he describes as difficult to navigate. Registering as a CQC manager also triggered an inspection that caught him off guard, though he says it proved less difficult than anticipated once it was underway.
Leadership brought its own realisation. Stressful days, he learned, have to be managed with care because the team takes its cue from the principal. “Your team mimics your persona and ethos,” he says, a line that frames leadership as something modelled rather than instructed. A costlier lesson came from due diligence. Dr Zain now wishes he had studied the practice’s services and equipment records more closely before completing. The gaps he later found led to investment he would not otherwise have chosen so early. He treats ownership as a long-term commitment rather than a quick return, one that asks for hours well beyond a 9-to-5, especially at the start.
Ownership surfaced something less practical and harder to plan for. “Practice ownership is sometimes a lonely experience,” he says, which is why he founded a Facebook group for practice owners, Diary of Dental Practice Owners. It is a deliberate piece of infrastructure, not a passing comment, and it points to a gap the profession rarely names.
Scaling: from clinician to entrepreneur
Dr Jin, Smile Clinic Group, became a principal at 23, straight out of foundation training, and now leads a team of more than 300 people. His early assumption was that clinical excellence would be enough to build a successful practice. Leadership, people and decision-making turned out to be the real challenges, since every choice affected patients, the team, the finances and the future at once. “Dental school prepares you to treat patients but not to run a business,” he says. Building systems and the right culture, he learned, drives long-term success more reliably than clinical skill alone.

Scale reshaped the financial lessons too. Turnover, he discovered, means little without strong cash flow, and unexpected costs can move performance more than any single decision. He now views every investment through the lens of return, whether it improves patient care, increases efficiency or supports growth. Managing people taught him a harder truth: one style never fits everyone, and “avoiding difficult conversations only creates bigger problems later.” Culture across 300 people, he has found, is built through communication, trust and accountability rather than written policy. Recruiting the right people beats trying to change the wrong ones.
His advice to associates is blunt. Do not wait until everything feels perfect, because that moment never arrives, and invest as much in business knowledge, leadership and communication as in clinical training. The furthest stage of the journey, in his account, is less about the practice and more about the organisation behind it.
Where the three stages meet
Read together, the three accounts split along two lines: how long each principal has held the role and how large the operation has grown. Dr Amisha is closest to the beginning, absorbing costs and dynamics that are still new. Dr Zain has moved past the initial shock and into building the systems and relationships that carry a single practice forward. Dr Jin has scaled a practice into a group and now manages leadership itself rather than day-to-day operations. One thread runs through all three, regardless of stage. The distance between what a plan projects and what a practice actually costs to run, in money, in trust, or in time, never closes completely. It only changes shape.
The entrepreneurial arc
Read as an entrepreneurial arc, the three stages line up cleanly. Founding is the highest-risk stage, defined by a steep learning curve and costs that only reveal themselves after the deal closes. Building is the derisking stage, where trust gets rebuilt, systems get tested and the practice starts to run on more than the principal’s instinct. Scaling is the stage where the job stops being about the practice at all and becomes about the people and structures running it. Dr Jin’s own framing captures the direction of travel: the principal who lasts learns to think like an entrepreneur rather than simply a clinician.
None of the three arrived at their stage ready for it, and each account suggests the profession spends more time preparing associates for the transaction than for what follows it. The legal checklist gets a practice through completion. What carries a principal through the years after is closer to what these three describe: reading costs correctly, rebuilding trust deliberately, and eventually leading people rather than treating patients. The transition does not end at any one stage. It compounds through all three.